Types of Delusions and How They Differ Across Mental Health Conditions
Introduction: Why Understanding Delusions Matters
Imagine believing something with your whole heart, even when everyone around you says it’s not true. That is what a delusion feels like for many people. Delusions are not the same as being stubborn, confused, or having a strong opinion. They are a real symptom of mental illness. And they affect more people than most realize.
Research shows that about 3% of people in the United States will experience psychosis at some point in their lives. Psychosis often includes delusions. In fact, delusions are a core feature of conditions like schizophrenia, bipolar disorder, and delusional disorder. These conditions fall under the broad severe mental illness definition. Studies on the lifetime prevalence of psychotic and bipolar I disorders help us understand just how widespread these experiences are.
Understanding the different types of delusions can make a real difference. It helps reduce the stigma around mental health.

It also makes it easier to spot the signs and symptoms of schizophrenia or related conditions early. Early recognition means people can get help sooner. And getting help early leads to better outcomes.
In this article, we will walk through the main types of delusions. We will also look at how they connect to conditions like bipolar schizoaffective disorder and what the psychosis ICD 10 codes mean. Whether you are living with these symptoms yourself or supporting someone who is, knowing what you are dealing with is the first step.
If you are new to learning about psychosis, you may want to read more about psychosis symptoms and why early recognition matters. It gives a clear starting point for understanding what to look for.
Let’s dive into the most common types of delusions and what makes each one unique.
What Are Delusions? A Clinical Definition
So what exactly is a delusion? The clinical definition might surprise you. According to the DSM-5, delusions are fixed beliefs that stay strong even when there is clear evidence against them. The belief does not change, no matter how much proof you show. The American Psychiatric Association describes them as false beliefs based on incorrect ideas about what is real. You can find the full DSM-5 definition of delusions outlined by mental health experts.
Here is the key: a delusion is not the same as being mistaken or confused. Everyone has wrong ideas sometimes. But a delusion is stuck.
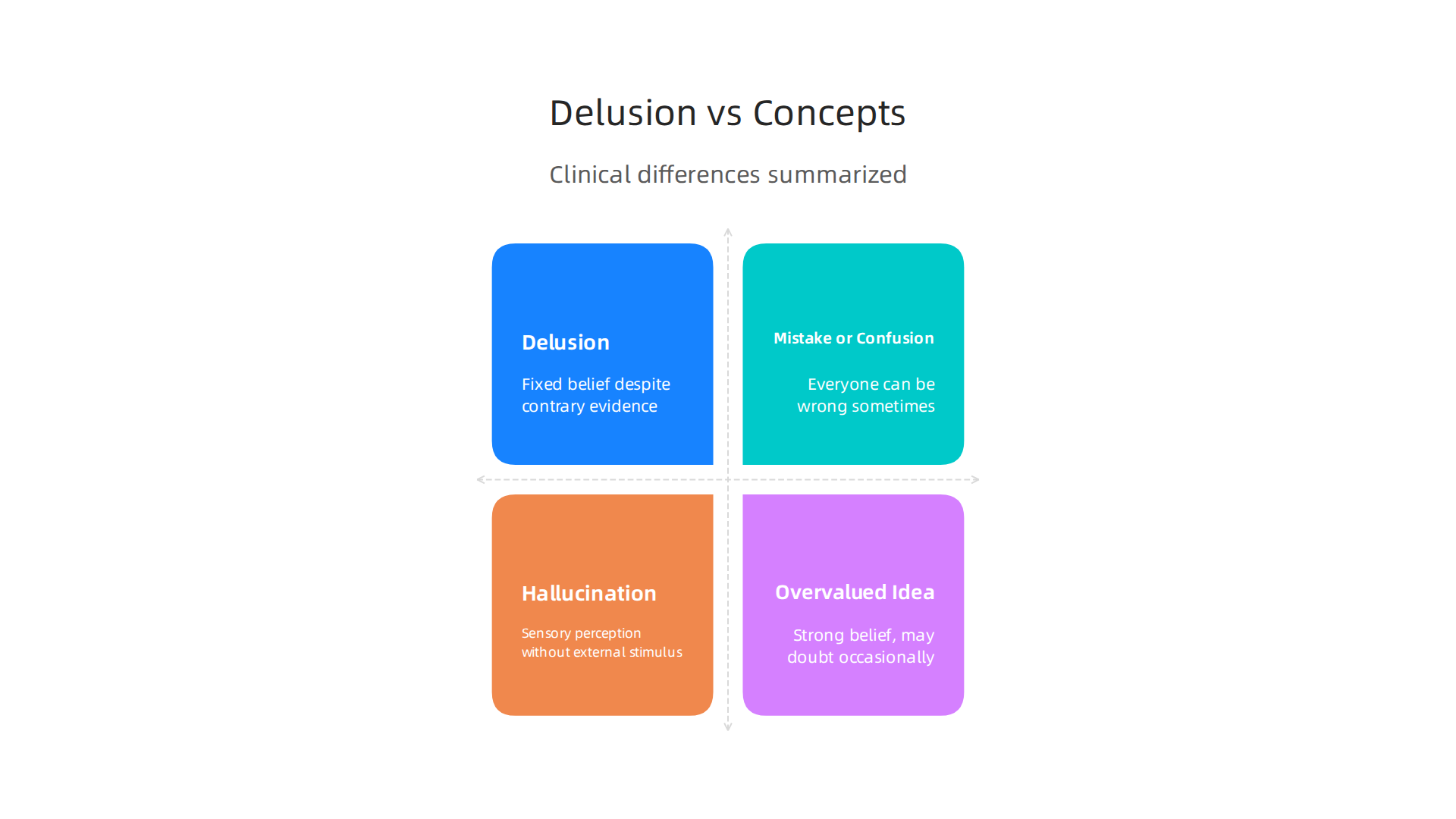
The person holds it with complete certainty. And it is not just a strong opinion or a cultural belief. For a belief to count as a delusion, it must not be something that other people in the person’s culture or religion normally believe. This is an important rule in the DSM-5. If a belief is part of a person’s cultural or religious background, it is not considered a delusion.
Delusions are also different from hallucinations. Hallucinations are sensory experiences without an outside cause. You might hear voices or see things that are not there. Delusions are not about sensing. They are about believing something that is not real. The professional guide from the MSD Manual on delusional disorder explains that delusions last for at least a month in delusional disorder, and the person may have no other psychotic symptoms.
Another way to think about it: delusions sit on a spectrum. They are more rigid than an "overvalued idea." An overvalued idea is a strong belief that you might question sometimes. A delusion is unshakable.
Understanding this clear definition helps you spot the difference between a weird thought and a real symptom. If you want to learn about related conditions where such fixed beliefs appear, you can read about paranoid personality disorder symptoms and causes. That condition involves suspicious thinking, but it is not the same as a full delusion. Knowing the boundaries gives you a better map of the mind.
The Major Types of Delusions: An Overview
Once you know what a delusion is, the next step is understanding the different forms it can take. Mental health professionals group delusions by their main theme. According to the DSM-5-TR definition of delusional disorder, the most common types include persecutory, grandiose, referential, and somatic delusions.
Persecutory delusions are the most frequent. The person believes someone is out to harm them, follow them, or spy on them. Grandiose delusions involve a false sense of special power, fame, or identity. Someone might believe they are a famous celebrity or have a secret mission. Referential delusions make the person think that ordinary events, like a news report or a stranger’s comment, are directly about them. Somatic delusions focus on the body. The person may believe they have a terrible disease or that their body has changed in some impossible way.
Other types include jealous delusions (believing a partner is unfaithful without reason) and erotomanic delusions (believing someone famous is in love with you). Understanding these patterns helps in spotting the early signs. This is especially true for conditions like schizophrenia, where the signs and symptoms of schizophrenia often include one or more of these delusion types. Each type has a different flavor, but they all share one thing: the belief is rigid and real to the person holding it.
Persecutory Delusions
Persecutory delusions are the most common type of delusion. People with these delusions believe they are being targeted by someone else. The threat might involve being followed, harassed, poisoned, or plotted against. According to the MSD Manual on delusional disorder, this type is especially frequent in paranoid schizophrenia. The belief feels completely real, even when there is strong evidence otherwise. This is different from normal suspicion or caution. The person may become very defensive. They might avoid people, refuse to go out, or stop trusting even close family members. Social withdrawal is a common outcome. Over time, the fear can take over their daily life. If you are trying to understand these experiences for yourself or someone you love, learning about paranoid personality disorder symptoms and causes can help because it shares some features with persecutory delusions.
Grandiose Delusions
Another key type of delusion is the grandiose delusion. People with this belief think they have special powers, fame, or a very high status. They might believe they are a famous celebrity, a religious figure, or an inventor of something world-changing. According to the DSM-5-TR definition of delusional disorder, these beliefs are fixed and not open to change. This type of delusion is very common in bipolar disorder during manic episodes. It can also appear in schizophrenia or schizoaffective disorder. A person might feel unstoppable or like they have a special mission. They may spend a lot of money or take big risks because of these beliefs. If you want to understand more about how mood affects these beliefs, learning about bipolar symptoms in women can help. Recognizing these types of delusions early is an important step toward getting the right support.
Referential Delusions and Other Common Types
Another common type of delusion is the referential delusion. People with this belief think that everyday events are directly aimed at them. A stranger’s cough might feel like a signal. A TV news story might seem like a coded message. These neutral moments take on deep personal meaning. According to the Delusional Disorder overview from Medscape, these beliefs are firmly fixed and cause real distress. Other types include somatic delusions (believing your body is diseased or not working right) and erotomanic delusions (believing someone famous or powerful is secretly in love with you). Delusions also fall into two groups. Bizarre delusions are clearly impossible, like your organs have been replaced by alien technology. Non-bizarre delusions could happen in real life, like being followed or poisoned. Knowing these types of delusions helps people spot warning signs early. If you want to understand more about related symptoms, learning about psychosis early recognition can be a helpful next step.
The Psychology and Neurobiology Behind Delusions
So why do delusions happen in the first place? It is not a simple answer. Researchers point to a mix of thinking patterns and brain chemistry working together.
One big piece is cognitive biases. These are mental shortcuts that go wrong. People prone to delusions often jump to conclusions with very little evidence. They also have trouble seeing things from another person’s point of view. This is called a theory of mind deficit. Research on cognitive biases and delusions in psychosis shows these thinking errors play a major role in forming fixed false beliefs.
Another piece is brain chemistry. The neurotransmitter dopamine acts like a signal booster in your brain. When the dopamine system in the mesolimbic pathway becomes overactive, everyday events start to feel too important. A car horn sounds like a warning just for you. A stranger’s laugh feels personal. A review on dopamine and cognitive biases in delusions explains how this chemical imbalance helps maintain delusions over time.
The good news is that understanding these brain mechanisms leads to better treatments. Therapies like CBT for psychosis help people spot their jumping-to-conclusions habit and slow it down.

If you want to learn more about helpful therapy approaches, check out this guide on cognitive behavioral therapy for anxiety for practical techniques.
This brain-based view also opens the door to newer ideas. For a deeper look at how behavioral mechanisms can shape recovery, the peer white paper called The Science of Gamification explains how structured reward systems can help shift these deep patterns.
Cognitive Biases in Delusion Formation
Let’s look at the specific thinking errors behind the types of delusions. We call these cognitive biases.
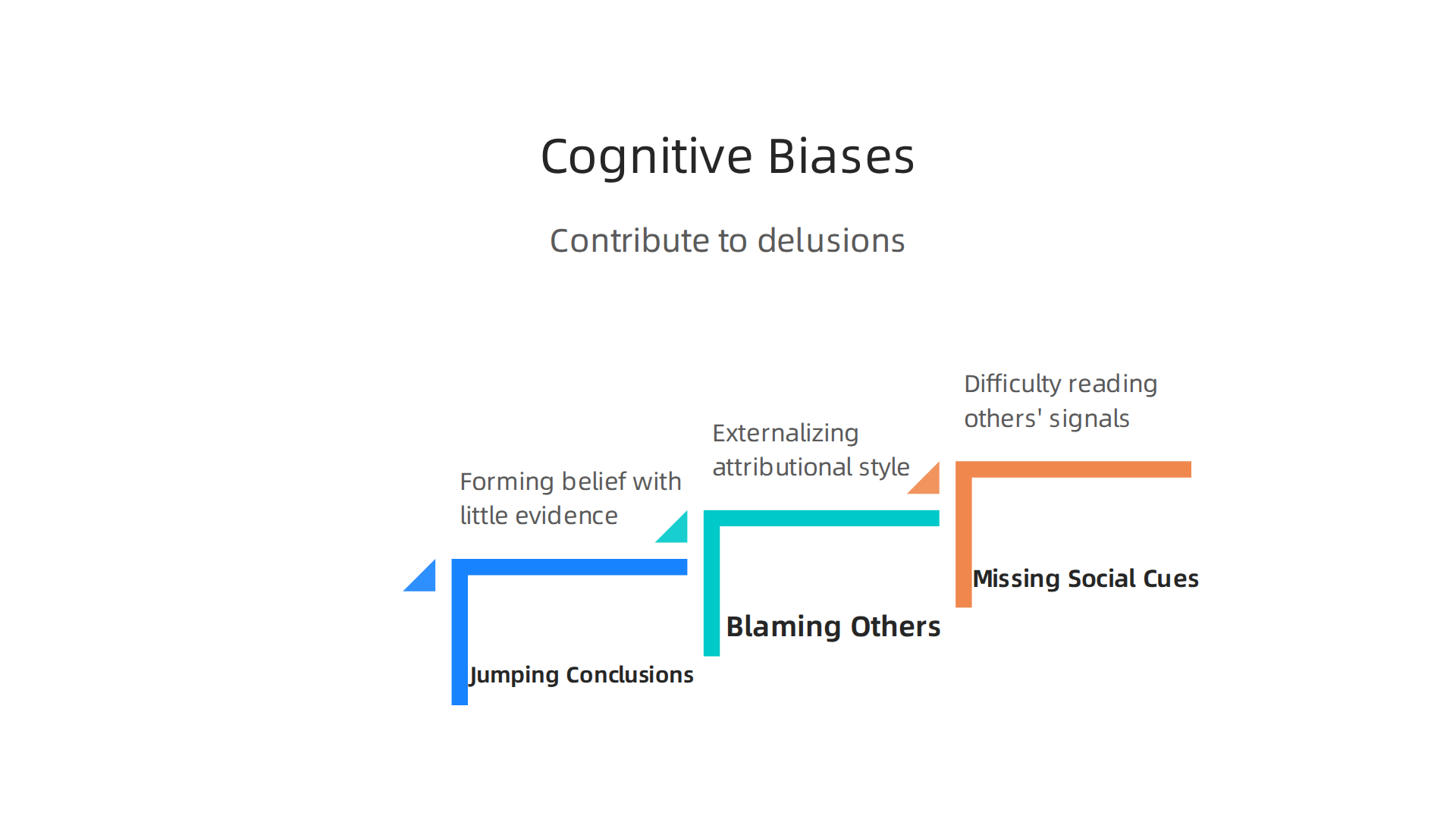
Jumping to conclusions. This bias means forming a strong belief with very little proof. A person might assume a coworker hates them just because of a missed greeting. Research on cognitive biases and decision-making in psychosis links this directly to early signs and symptoms of schizophrenia.
Blaming others. People with this bias automatically blame others for negative events. This is called an externalizing attributional style. It feeds paranoid thinking and is a common feature of conditions under the psychosis icd 10 classification.
Missing social cues. This is a theory of mind deficit. The person struggles to understand that others have separate thoughts and feelings. A simple look can feel like a threat. This is common in bipolar schizoaffective disorder. For more on how these patterns look in daily life, see this overview of paranoid personality disorder symptoms.
These biases are not random. They are predictable thinking errors. Understanding them moves us beyond simple labels. It shows that delusions follow a logic, even if that logic is broken. This fits the severe mental illness definition, where thinking patterns are deeply distorted. And it opens the door to treatments that target how a person thinks, not just what they think.
Neurobiological Vulnerabilities
Cognitive biases are one piece of the puzzle. The other piece is what happens in the brain itself. Scientists have found clear links between certain brain differences and the types of delusions people experience.
Too much dopamine. The striatum is a deep brain area involved in reward and motivation. When it releases too much dopamine, everyday events can feel overly important. This is called aberrant salience. A neutral sound or glance suddenly feels loaded with meaning. This dopamine disruption is a well-known feature of psychotic disorders and is part of the psychosis icd 10 classification. For more on the dopamine model, see this review on dopamine and cognitive biases in delusion formation.
Prefrontal cortex trouble. The front part of your brain helps you test reality. It lets you check: "Is this belief reasonable?" When the prefrontal cortex is not working well, a person has a harder time questioning their own thoughts. This makes it easier for false beliefs to stick.
Genes and environment meet. These brain vulnerabilities do not come out of nowhere. Genetics can make someone more prone to dopamine problems. Then life stress or cannabis use can push that person over the edge. This gene environment interaction is a core idea behind the severe mental illness definition.
Understanding these brain changes helps explain why delusions are not just "bad thinking." They have a biological basis. And that means biological treatments can help too. If you want to learn more about early warning signs, check out this guide on psychosis symptoms and early recognition.
How Delusions Differ Across Mental Health Conditions
Not all delusions look the same. The types of delusions someone experiences often depend on the specific condition they have. Understanding these differences helps with accurate diagnosis and better treatment.
Schizophrenia and bizarre delusions. In schizophrenia, delusions tend to be strange and hard to believe. A person might think aliens have planted a microchip in their brain. Or that their thoughts are being broadcast on the radio. These beliefs are often fixed and long lasting. They are a core part of the signs and symptoms of schizophrenia. The brain changes we talked about earlier, like too much dopamine and prefrontal cortex trouble, play a big role here.
Bipolar disorder and mood tied delusions. In bipolar schizoaffective disorder and bipolar I disorder, delusions usually match whatever mood state the person is in. During mania, delusions are often grandiose. Someone might believe they are a famous celebrity or that they have special powers. During depression, delusions turn dark. People might believe they have committed a terrible crime or that they are being punished. This connection between mood and belief is a key clue for doctors. For more on how bipolar symptoms show up, check out this guide on bipolar symptoms in women.
Delusional disorder: non-bizarre but persistent. This condition is different. The delusions are not bizarre at all. They could actually happen in real life. A person might believe their spouse is cheating on them or that the government is watching them. These beliefs last for a month or longer. But the person does not show other psychotic symptoms like hallucinations. This makes delusional disorder harder to spot because the person might seem perfectly normal otherwise. Research shows that cognitive biases like jumping to conclusions are especially common in this group. For a deeper look at how these biases work, see this study on Relationships between cognitive biases, decision-making.
Understanding how delusions differ across conditions is not just academic. It helps therapists and doctors choose the right treatment. And it helps families understand what their loved one is going through.

Recognizing these patterns can reduce confusion and open the door to real help. As research on shaping healthy behaviors shows, understanding your own patterns is the first step toward change. A platform that tracks and rewards positive behaviors can be a powerful tool for mental health. Check out how Authority Magazine highlighted this approach for offsetting anxiety and depression.
Recognizing Delusions in Yourself or Others
One of the hardest parts about delusions is spotting them early. Whether you are concerned about yourself or someone you care about, knowing what to look for can make a real difference.
Early warning signs to watch for. People who are developing delusions often start acting differently. They might become more suspicious of others for no clear reason.

They may talk about beliefs that seem unrealistic or impossible. Another common sign is pulling away from friends and family. Someone who used to enjoy social time might start staying home alone. These changes can be gradual, so paying attention to patterns matters.
Check if the belief fits the culture. Not every unusual belief is a delusion. Sometimes a belief is part of a person’s cultural or religious background. The key question is whether the belief causes distress or gets in the way of daily life. A person who thinks their neighbor is spying on them might still be able to work and keep friendships. But if that belief stops them from leaving the house, it is a problem. This idea of checking function is part of the severe mental illness definition that doctors use.
Create a safe space to talk. People with delusions often feel scared or confused. They might not tell anyone what they believe because they think others will not understand. If you want to help, listen without arguing. Do not tell someone their belief is wrong. Instead, say something like, "I can see this feels very real to you." This kind of support makes it easier for them to open up and get help sooner. Professionals use tools like the PANSS Scoring & Interpretation scale to measure how severe symptoms are and guide treatment.
If you are worried about a loved one, learning more about early signs is a great first step. Check out this guide on psychosis symptoms why early recognition matters for more details.
Recognizing delusions early opens the door to real change. The right support and habits can make a big difference. The Youth Safety Case Study shows how tracking healthy behaviors builds resilience and helps people resist negative thought patterns.
Diagnosis: How Clinicians Assess Delusions
Getting an accurate diagnosis is a careful process. Doctors don’t just ask if someone has strange beliefs. They use specific tools and a thorough approach to understand what is really going on.
Structured interviews are the gold standard. The most common tool is the Positive and Negative Syndrome Scale, or PANSS. It has 30 items that measure the severity of psychotic symptoms. Another key tool is the SCID-5, a structured interview that helps doctors make a clear diagnosis. One study described the SCID-PANSS two-tier diagnostic system as a way to combine diagnosis with a deeper look at how symptoms affect daily function.
What doctors look for. When a clinician assesses delusions, they need to know a few things. When did the belief start? How strong is the person’s conviction? Does the belief get in the way of work, relationships, or self-care? These details help separate a passing odd thought from a serious delusion that needs treatment.
Ruling out other causes comes first. Not every false belief is a mental health condition. Doctors must check for medical issues that can look like delusions. Things like dementia, brain injury, or substance use can cause similar symptoms. A full medical exam is part of the process.
If you want to understand the bigger picture of how these symptoms fit together, reading about bipolar schizoaffective disorder can help clarify the differences.
Treatment and Management Approaches for Delusions
Once a doctor confirms a diagnosis, the next step is finding the right treatment. Getting help early makes a big difference. Knowing the specific types of delusions a person experiences helps doctors choose the best treatment plan.
Antipsychotic medications are the first line of defense. These drugs change brain chemistry to reduce delusions and other psychotic symptoms. They work best when started early and taken consistently. The efficacy of second-generation antipsychotics has been confirmed in many studies, with medications like clozapine and risperidone showing strong results. Doctors often try one medication, then adjust based on how the person responds and what side effects they experience.
Therapy also plays a key role. Cognitive Behavioral Therapy for psychosis, or CBTp, helps people challenge and cope with delusional beliefs instead of just reacting to them. This approach builds on behavioral science principles, and resources like The Science of Gamification explain how these mechanisms work in practice. CBTp is not about arguing someone out of a delusion. It is about learning to notice the belief, test it gently, and reduce the distress it causes.
Family support and education improve long-term outcomes. When family members understand what delusions are and how treatment works, they can offer better support. Learning about early recognition of psychosis symptoms helps families spot early warning signs and act quickly. This kind of teamwork between doctors, patients, and families leads to fewer relapses and a better quality of life.
The Role of Psychosocial Interventions
Medication alone is rarely enough. Psychosocial interventions help people with delusions rebuild their lives. These treatments focus on thoughts, skills, and daily functioning.
Cognitive Behavioral Therapy for psychosis (CBTp) is one of the most effective approaches. It helps people examine their delusional beliefs without judgment.
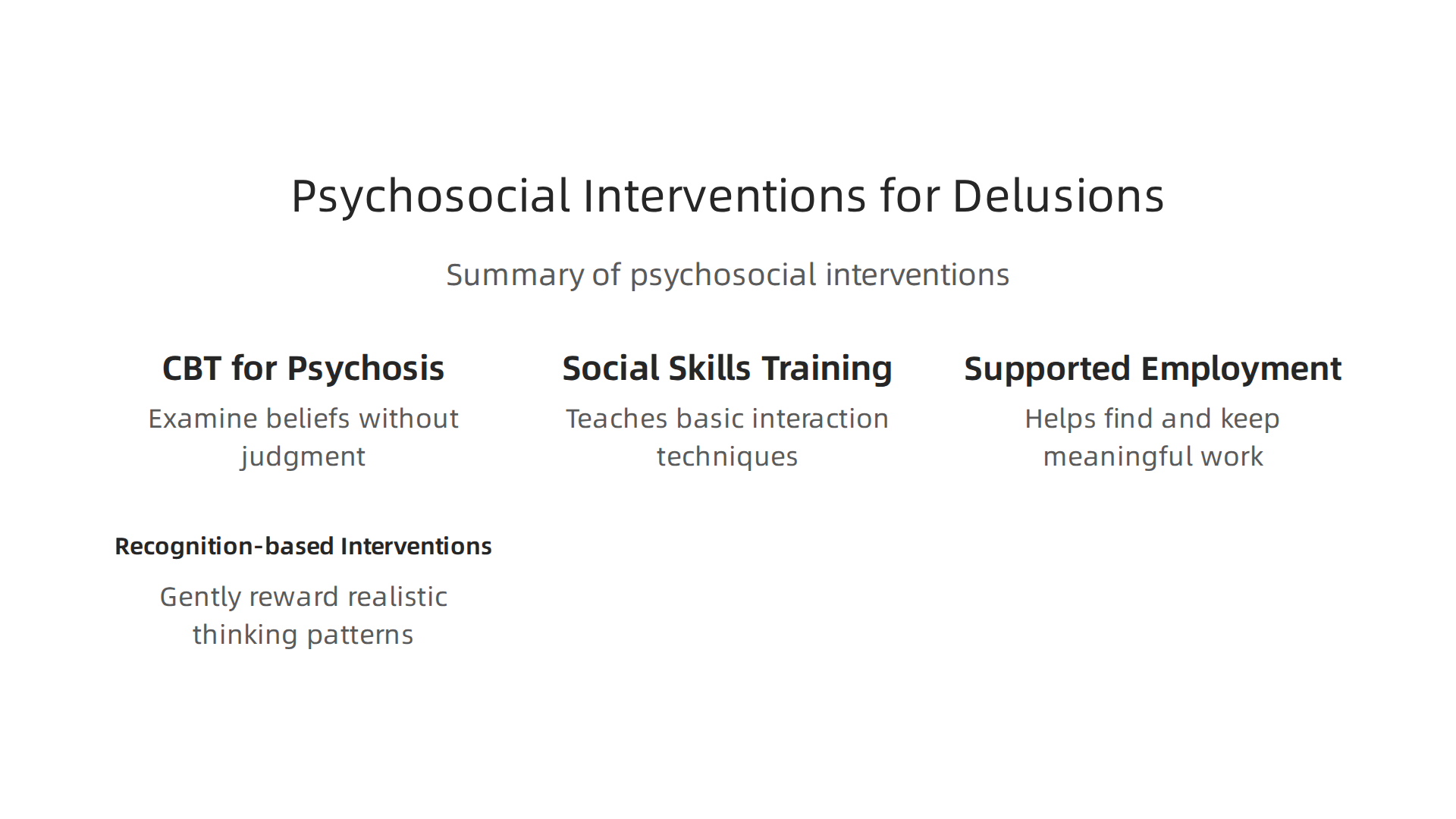
Over time, the conviction behind the delusion weakens, and the distress it causes drops. This is not about proving the belief wrong. It is about learning to live with less fear.
Social skills training and supported employment target the practical problems that come with severe mental illness. Many people struggle to communicate, hold a job, or manage daily tasks. Social skills training teaches basic interaction techniques. Supported employment helps people find and keep meaningful work. Both improve quality of life.
Recognition-based interventions like the Video Reinforcement Survey (VRS) take a different path. They gently reward realistic thinking patterns. When a person accurately perceives reality, the VRS reinforces that thought. Over time, this can reduce false beliefs.
These interventions work best when combined with medication and family support. A recent systematic review on antipsychotic effectiveness and quality of life shows that combining medication with psychosocial care improves outcomes. To learn how similar techniques apply to other conditions, read about paranoid personality disorder symptoms causes and treatment options.
Summary
This article explains what delusions are, why they matter, and how to recognize and respond to them. It opens with a clear DSM-based definition and prevalence context, then describes the major types of delusions — persecutory, grandiose, referential, somatic, jealous, and erotomanic — and how they present. The piece reviews thinking errors and brain changes (cognitive biases, dopamine, prefrontal dysfunction) that create and maintain delusions, and it shows how delusions differ in schizophrenia, bipolar-related illnesses, and delusional disorder. It outlines how clinicians evaluate delusions (SCID, PANSS, medical workup) and summarizes evidence-based treatments including antipsychotic medication, CBT for psychosis, family education, and psychosocial rehabilitation. Practical guidance for spotting early warning signs and talking with someone who holds a delusional belief is included, emphasizing early recognition and combined care for better outcomes.