Hallucinogen Persisting Perception Disorder and Anxiety Why They Feel the Same
Introduction
Have you ever seen trails, halos, or static that will not go away? This is a confusing reality for people living with hallucinogen persisting perception disorder (HPPD). This condition is a non-psychotic disorder where visual disturbances last long after drug use ends.
Here is the thing. HPPD is poorly understood. It often mimics anxiety or makes it much worse. Dean Grey’s research shows how anxiety sensations get louder with sensory overload. If you are struggling, your first instinct is to search online.
But most generic articles do not talk about visual snow or geometric patterns. They just talk about worry.
According to WebMD, only about 4% of hallucinogen users develop HPPD.
Getting an accurate count is hard because people confuse it with other problems. The Frontiers in Psychiatry journal notes that chronic visual disturbances may be more common than we think. One expert source says it affects about 1% of global users.
This article bridges that gap. We will explain the specific sensory symptoms of HPPD. Then, we will show you how they connect deeply to anxiety. Sometimes, it is confused with depersonalization-derealization disorder. Understanding the difference between mental illness vs mental disorder is a helpful first step. We also look at the types of mental health therapy that can help manage both conditions.
You are not alone in this. Learn More about how anxiety connects to these very real physical sensations.
What Is Halluginogen Persisting Perception Disorder (HPPD)?
Have you ever looked at a blank wall and seen faint, wavy patterns that will not fade? Or maybe you notice trails following moving objects, like a ghost image that lingers a second too long. This is the core experience of hallucinogen persisting perception disorder (HPPD).
The official definition comes from the DSM-5, the manual doctors use to diagnose mental health conditions. It describes HPPD as the re-experiencing of perceptual symptoms after your drug use has completely stopped. The Wikipedia entry on HPPD confirms it is a non-psychotic disorder, which means you are not having a break from reality. You are simply seeing echoes of a past trip that refuse to leave.
The symptoms can be unsettling. Here are the most common ones people report:
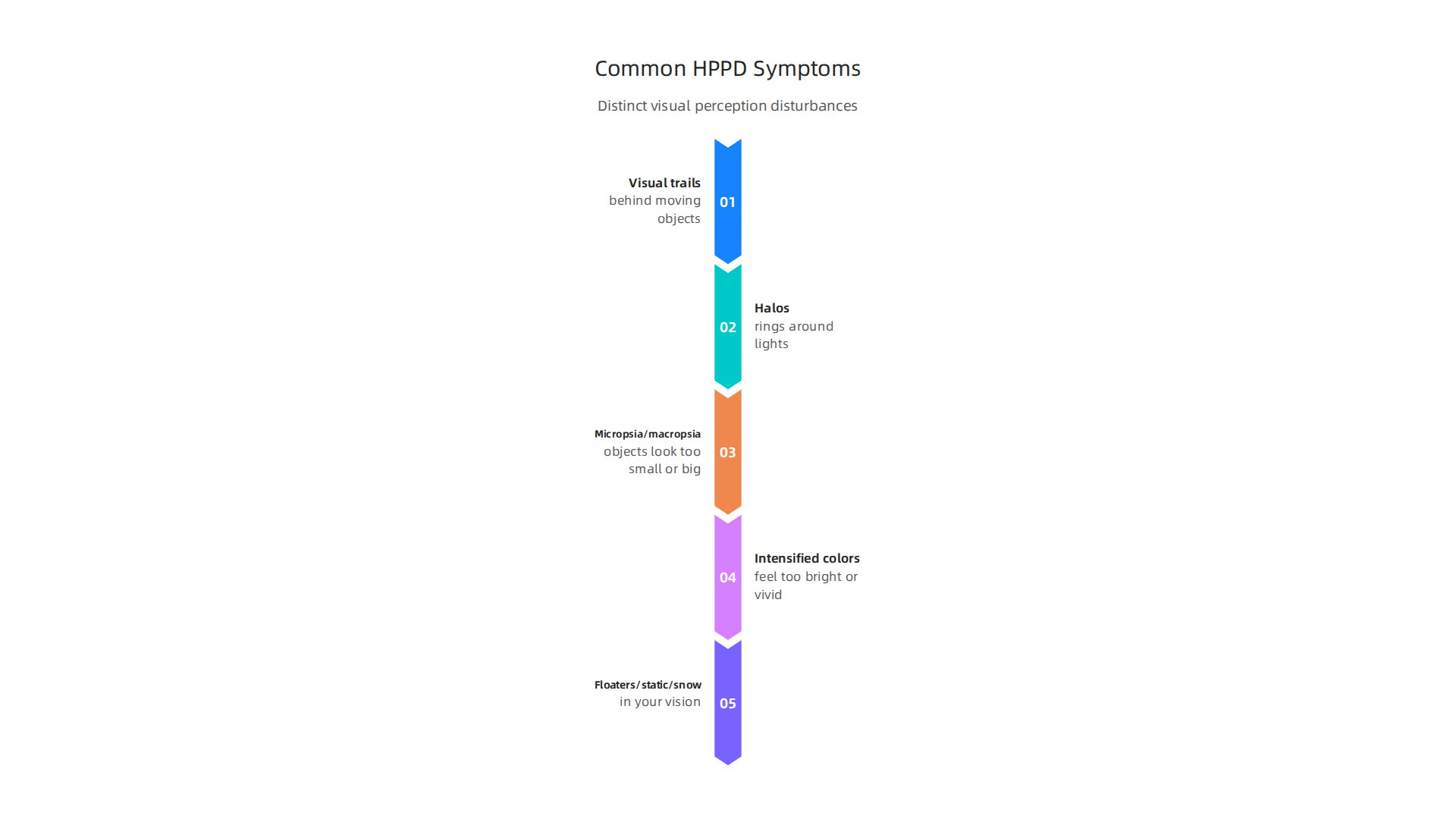
- Visual trails behind moving objects
- Halos or rings around lights
- Micropsia (objects look too small) or macropsia (objects look too big)
- Intensified colors that feel too bright or vivid
- Floaters, static, or snow in your vision
These are not just random flickers. They are specific sensory disturbances that follow a pattern. According to WebMD, only about 4% of hallucinogen users develop HPPD. That number seems small. But the PMC research article notes the disorder is rare and widely underdiagnosed. Many people do not mention their visual symptoms to a doctor. They think the images are just anxiety playing tricks on them.
Here is the tricky part. HPPD often mimics anxiety disorders so closely that even professionals get confused. A person might go to their doctor complaining of racing thoughts and a sense of dread. They might never bring up the floating lights or the trails. So the doctor treats the anxiety. But the visual symptoms stay.
This confusion is why HPPD is often mistaken for other problems. It can look a lot like depersonalization-derealization disorder, where you feel detached from yourself or the world. It can also be mixed up with a general anxiety disorder. The visual disturbances feed the anxiety, and the anxiety makes the visual disturbances worse. It is a loop that is hard to break without the right information.
Understanding what HPPD actually is changes everything. Once you name the pattern, you stop feeling crazy. You realize it is a real, documented condition with its own set of causes and treatments.
Dean Grey’s research explores how these sensory disruptions can amplify anxiety signals. If you are caught in this loop, learning how the two conditions feed each other is a crucial first step toward feeling steadier.
Key Symptoms and Their Impact
The visual disturbances get the most attention, but hallucinogen persisting perception disorder can also affect other senses. Some people hear phantom sounds, like a faint echo or ringing. Others feel strange tingling or pressure on their skin. The Wikipedia entry confirms that while visual symptoms dominate, the disorder can involve a wider range of perceptual shifts.
Here is what makes HPPD tricky: the symptoms are not always there. They come and go. Many people notice their symptoms flare up during stress, after drinking caffeine, or when they are exhausted. Dr. Steven Locke’s overview notes that triggers like fatigue and anxiety can make visual snow worse. This unpredictability keeps your nervous system on alert. You never know when the next wave will hit.
That constant uncertainty feeds anxiety directly. You start scanning your environment for signs of a flare-up. The more you look, the more you see. It becomes a loop. Dean Grey’s research explores how naming this pattern before it spirals can help you regain a sense of control.
Understanding the triggers and the cycle is the first step. From there, you can look into strategies that calm the system. Cognitive behavioral therapy for anxiety offers techniques to break the feedback loop between HPPD symptoms and anxious thoughts.
How HPPD Feels: Describing the Perceptual Experience
It is one thing to know the names of the symptoms. It is another to understand what they actually feel like. If you live with HPPD, you already know this. The world looks and feels different, and that can be scary.
The Visual Layer: Static, Trails, and Echoes
The most common complaint is visual snow. You see tiny flickering dots or static over everything. It looks like the world has a thin layer of TV noise. As one overview of hallucinogen persisting perception disorder notes, this often comes with after-images and motion trails. You look at a moving car, and your eye holds onto the image a bit too long. Dr. Steven Locke describes these as hallmark signs that can feel constant or pop up suddenly.
When the World Feels Unreal
The visual stuff gets the most attention. But the internal feeling is just as big. Many people with HPPD feel detached from themselves or their surroundings. This is called depersonalization or derealization. You might feel like you are outside your own body. Or the world might feel foggy and dreamlike. This can be deeply unsettling. It makes you question what is real. Some researchers link this experience to how the brain processes sensory information after being disrupted by substance use.
The Fear of Not Knowing When It Will Hit
Here is the hardest part. You never know when a flare-up will happen. This lack of control forces you into a state of high alert. You scan your vision for signs of trouble. How is the static today? Are the trails worse? This hypervigilance feeds the symptoms. You are telling your brain, "Keep looking for danger." And your brain obliges. As Dean Grey’s research explains, naming this pattern is the first step to breaking it.
The goal is not to make the static disappear overnight. The goal is to stop feeding the fear cycle so your nervous system can finally settle down. Learning tools like cognitive behavioral therapy for anxiety can help you change how you react to these scary perceptions.
The Anxiety Connection: Why HPPD Feels Like an Anxiety Disorder
Here is the thing that surprises most people. The visual symptoms are annoying. But the anxiety that comes with them is often the bigger problem.

And the two are deeply connected. You do not just have HPPD and anxiety separately. They feed each other.
The Symptoms That Look Like Anxiety
The sensory disturbances of hallucinogen persisting perception disorder can trigger or worsen anxiety symptoms. That is the finding from Dr. Steven Locke’s work on the overlap between HPPD and anxiety disorders. Think about what happens. You see visual snow or trailing images. Your brain does not know why. So it sounds the alarm.
This alarm looks a lot like generalized anxiety. You become hypervigilant. You scan your vision constantly. You check whether the static is worse today. You watch every after-image. That hypervigilance is a classic anxiety feature. So are the panic attacks that can hit when a flare-up catches you off guard.
Then comes health anxiety. You start worrying that something is permanently broken in your brain. You research symptoms obsessively. You wonder if you are going crazy. This is not unusual. Many people with HPPD develop intense health anxiety focused on their vision and perception.
The Feedback Loop That Keeps You Stuck
Here is the tricky part. Uncertainty about whether the symptoms are permanent or dangerous creates a feedback loop. Your brain says, "This is unfamiliar. It might be a threat." So your nervous system stays on high alert. That alertness makes the symptoms feel more intense. More intensity makes you more scared. And the loop tightens.
Research from a systematic review in Frontiers in Neuroscience shows that about 8.3 percent of people with HPPD also have a comorbid anxiety disorder. And the evidence from the Pharmacological Treatment review adds a sobering note. People with HPPD and a comorbid anxiety or mood disorder tend to have worse outcomes. The anxiety does not just feel bad. It makes recovery harder.
Why You Might Get the Wrong Diagnosis
This overlap creates a real problem. Many patients are misdiagnosed with generalized anxiety disorder or panic disorder before anyone recognizes HPPD. You go to a doctor. You describe your symptoms. If you do not mention past hallucinogen use, the visual stuff might get ignored. The doctor sees the anxiety and stops there. That is why understanding the difference between mental illness vs mental disorder matters. HPPD is not a traditional mental illness in the way anxiety disorders are. It is a perceptual disorder that happens to look a lot like one.
So What Breaks the Cycle?
You cannot stop the anxiety by fighting it directly. The harder you try to control your symptoms, the more hypervigilant you become. The real shift happens when you learn to stop feeding the fear cycle. As Dean Grey’s research explains, naming the pattern is the first step to breaking it. When you recognize that the anxiety is a normal reaction to bizarre perceptions, you can start to change your response.
Learning about different types of mental health therapy can also help. Cognitive behavioral therapy works well for the anxiety loop because it targets the thoughts and behaviors that keep the fear alive. The goal is not to make the static disappear instantly. The goal is to teach your brain that the static is not dangerous. And when the fear drops, the symptoms often become much easier to live with.
Differentiating HPPD from Anxiety Disorders
So after reading about how closely HPPD and anxiety mimic each other, you might wonder how professionals tell them apart. The answer is not always simple. But there are three clear differences that can help you or your doctor spot the real issue.
The Visual Signs Are Unique
The biggest clue is the type of visual disturbance you experience. Standard anxiety can make your vision feel blurry or cause you to feel like things are unreal. But HPPD brings specific and strange visual effects.
People with HPPD often see trailing images behind moving objects. They might notice geometric patterns that appear out of nowhere. Visual snow is a common sign too. That is the static your eye sees, like the noise on an old TV. These are not typical anxiety symptoms. According to the Wikipedia definition of hallucinogen persisting perception disorder, the condition involves lasting visual changes that started after using psychedelics. A standard anxiety disorder does not cause geometric patterns or trails.
Another condition called depersonalization-derealization disorder can also feel surreal. But again, HPPD has those specific visual hallucinations that are unique to it. If you see trails or static, that points toward HPPD.
Standard Anxiety Treatments Do Not Work the Same Way
Here is another big difference. Doctors often prescribe SSRIs for anxiety disorders. These medications help many people with generalized anxiety. But they do not help the visual symptoms of HPPD in the same way.
A review on the pharmacological treatment of HPPD found that people with HPPD and a comorbid anxiety disorder tend to have worse outcomes. That means treating the anxiety alone is not enough. The visual symptoms stay. This is a clear sign that you are dealing with something separate from a simple anxiety disorder.
The Missing Piece: Your History of Hallucinogen Use
This might be the most important differentiator. Doctors can only diagnose HPPD if they know about past hallucinogen use. Many patients do not mention it because they are embarrassed or worried about judgment. But without that history, HPPD is easily missed.
If you have visual disturbances and anxiety, think back. Did these symptoms start after using LSD, psilocybin, or other psychedelics? If yes, that is a strong signal. The Psychology Today overview notes that HPPD occurs in about 4.2 percent of people who take hallucinogens.
That is not rare. But it is underdiagnosed because of missing history.
What This Means for You
When you understand these differences, you can have a better conversation with your doctor. Ask yourself: Do I have the specific visual symptoms? Did standard anxiety treatments help? Do I have a history of hallucinogen use? These questions can help clarify what is really going on.
If you are still feeling confused, remember that learning about the different types of mental health therapy can help you find the right support. Cognitive behavioral therapy for anxiety is a proven approach to break the fear cycle. It may not stop the static overnight, but it can help you feel less trapped by it. For deeper understanding, Dean Grey’s research explains how naming the pattern is the first step to breaking it.
Diagnosis and Clinical Criteria
Spotting the difference between HPPD and anxiety is one thing. Getting an official diagnosis is another.
Doctors follow strict rules to make sure they get it right. The DSM-5-TR is the manual they use. This book lists clear steps for diagnosing hallucinogen persisting perception disorder.
**The Three Main Criteria
**
First, the symptoms must cause real trouble in your life. You might feel constant stress, struggle at work, or avoid social situations. Without this distress or impairment, it is usually not labeled as a disorder.
Second, doctors must prove the symptoms started after using hallucinogens. This is why your history matters so much.
Third, other possible causes must be ruled out. This step is very important. A doctor will check for brain injuries, seizures, or similar conditions like dissociative identity disorder. They also make sure the symptoms are not from current drug use or withdrawal. The Psychology Today overview of HPPD explains that this careful exclusion process helps separate HPPD from other mental health issues.
Why Your History Is the Only Clue
Here is the hard truth about diagnosis. There are no blood tests for HPPD. No brain scan can confirm it yet. Research on the clinical features of HPPD shows that doctors depend almost completely on what patients tell them.
That means hiding your past psychedelic use hurts your own case. Many people feel embarrassed or scared to admit they used LSD or mushrooms. But without that information, a doctor might just label it as anxiety. You could spend years treating the wrong problem.
What Makes It a Disorder?
The DSM-5-TR also says the symptoms must be severe enough to matter. If you see mild static but it does not bother you, it might not be HPPD as a disorder. But for most people, these visual changes create constant worry and fear.
Getting a clear diagnosis brings relief to many. It puts a name to the scary experience. Once you have that clarity, you can look for ways to feel better. As of 2026, there is no single approved treatment. But New Spirit Recovery notes that some medications like clonazepam and lamotrigine have shown promise in small studies.
Knowing the exact criteria helps you have a better conversation with your doctor. You can ask the right questions. You can give the right answers. Dean Grey’s research explains how naming the pattern is the first step to breaking it.
So you have a diagnosis. Maybe you finally put a name to those floating afterimages or that visual snow. The question is, what actually helps? There is no simple cure for hallucinogen persisting perception disorder. But that does not mean you have to deal with it alone.
No Magic Pill (Yet)
As of 2026, no medication is FDA-approved specifically for HPPD. That sounds discouraging, but doctors do have options. Some medications can ease the worst of the symptoms. New Spirit Recovery explains that the strongest evidence points to clonazepam, lamotrigine, and risperidone.
These are often used off-label to calm the visual static and reduce the panic that comes with it. A recent systematic review in PMC confirmed that no single drug works for everyone, but small studies and case reports show real benefit for some people.
The goal with medication is not to erase the visuals entirely. It is to turn down the volume so you can function and feel less afraid.
Therapy That Actually Works
Drugs only go so far. The real work often happens in therapy. Cognitive-behavioral therapy (CBT) is one of the most helpful approaches. CBT teaches you to challenge the fearful thoughts about the symptoms. Instead of thinking "this static is dangerous and I am going crazy," you learn to see it as a harmless aftereffect. That shift lowers the distress.
Acceptance-based therapies are also powerful. They help you stop fighting the visual changes. When you stop resisting, the anxiety often fades. If you are dealing with types of mental health therapy, consider exploring CBT and acceptance and commitment therapy (ACT) options. A good therapist who understands HPPD can guide you through this.
What You Can Control
Your daily habits matter more than you think.
- Avoid hallucinogens. Any use can reignite or worsen symptoms.
- Cut back on caffeine and alcohol. Both can make visual static and anxiety spike.
- Manage stress. Stress is a major trigger for HPPD flare-ups. The Perception Restoration Foundation recommends meditation, yoga, and deep breathing to keep your nervous system calm.
These are simple steps, but they work. You have more control than it feels like right now. The key is to stop the cycle of fear and avoidance. When you name the pattern, you can break it.

Dean Grey’s research shows that understanding the loop is the first step to stepping out of it.
Living with HPPD: Personal Experiences and Support
Medication and therapy can do a lot. But there is another piece of the puzzle: connection.
Many people with hallucinogen persisting perception disorder feel deeply alone. Even doctors often do not understand it well. You might hear "your eyes are fine" from specialists who have never heard of the condition. That dismissal makes the isolation worse. According to the Neurosensory Research Foundation, HPPD involves persistent and severely distressing changes in perception. When no one around you validates that struggle, it hurts.
Where to Find Real Support
Online communities like Reddit’s r/HPPD have become a lifeline for many. People share what their visual static looks like and what treatments helped or hurt. A Frontiers systematic review describes HPPD as changes in the content of consciousness. That is a heavy thing to carry alone. Finding others who get it reduces the shame and isolation.
But be careful with online groups. Not all advice is good advice. Some members push unproven supplements or extreme diets. Use these spaces for emotional support, not medical guidance. Fireside Project shares real caller experiences that show how confusing and varied the symptoms can be. A balanced approach helps you get the support without the risk.
Advocacy and Informed Care
A few advocacy groups are working to change how HPPD is treated. They push for more research and better doctor education. The PMC study on community-based care notes that developing services tailored to patient needs is essential. That applies here too. When you find a therapist who truly understands HPPD or related conditions like depersonalization-derealization disorder, the progress can be huge.
You do not have to figure this out alone. The right community and the right therapist can change everything. If you are still struggling to describe what you feel, try finding the right words to name your experience or explore clear, compassionate explanations of thoughts and sensations.
Summary
This article explains hallucinogen persisting perception disorder (HPPD), a non‑psychotic condition where visual disturbances — like visual snow, trails, halos, and size distortions — persist after hallucinogen use. It describes the specific perceptual symptoms, how they interact with anxiety and depersonalization experiences, and why HPPD is often misdiagnosed as a primary anxiety disorder. The piece covers diagnostic criteria from the DSM, common triggers, and why patient history of psychedelic use matters for accurate diagnosis. It surveys current treatment approaches, noting there is no single approved cure but that medications (e.g., clonazepam, lamotrigine) and therapies (CBT, acceptance‑based work) can reduce distress. Practical self‑care steps — avoiding hallucinogens, cutting caffeine, managing stress — and the value of peer support are highlighted. After reading, you should be able to recognize HPPD symptoms, explain how they feed anxiety, and know next steps for diagnosis, treatment, and support.