Dissociative Identity Disorder Symptoms Causes and Treatment Options
Have you ever felt like there are different versions of you inside?

For many people, that feeling is just a passing thought. But for others, it is a daily reality called dissociative identity disorder (DID).
DID affects about 1.5% of the general population. That is not rare. In fact, studies from the National Institutes of Health show it is as common as other well-known mental health conditions. Yet it remains one of the most misunderstood.
Why? Because many people with DID go undiagnosed for years. Their symptoms get confused with other issues like depression or borderline personality disorder symptoms. They might not even know that therapists for dissociative identity disorder exist. According to experts at Psychiatry.org, dissociative disorders involve problems with memory, identity, and sense of self. This confusion can feel really lonely.
If you are trying to understand your own mind, you are not alone. Feeling pressure to figure it all out at once can make things harder. Behavioral Scientist Dean Grey studies how this pressure builds inside us. Sometimes, learning simple patterns helps.
And if you are struggling with intense fear or overwhelm, tools like Cognitive Behavioral Therapy can offer a lifeline. It is a proven way to calm a racing mind.
This article is here to give you a clear, full picture. We will cover the real definition, the signs, and how treatment works. Our hope is that you walk away feeling more informed and less alone. If this sounds helpful, subscribe to our newsletter for more plain-language guides.
What Is Dissociative Identity Disorder?
Let’s start with a clear definition. Dissociative identity disorder (DID) is a psychiatric condition where a person has two or more distinct personality states or identity fragments. These are not just "moods" or "sides of your personality." Each state can have its own way of thinking, memories, and even physical responses. The DSM-5-TR, which is the main guide doctors use, describes this as a disruption of identity where these states take control of behavior at different times.
You might have heard the old name "multiple personality disorder." That label was changed in the DSM-IV back in 1994. The new name, dissociative identity disorder, puts the focus on what is really happening: a split or dissociation in the sense of self. Researchers explain that this is not about having extra personalities. It is about a mind that could not fully integrate into a single identity during childhood. One review notes that each identity can have unique traits, memories, and life stories.
Here is the part that matters most. DID almost always comes from severe, repeated trauma in early childhood. When a young child faces overwhelming abuse or neglect, their brain does not have a mature way to cope. So it creates separate compartments for different experiences.
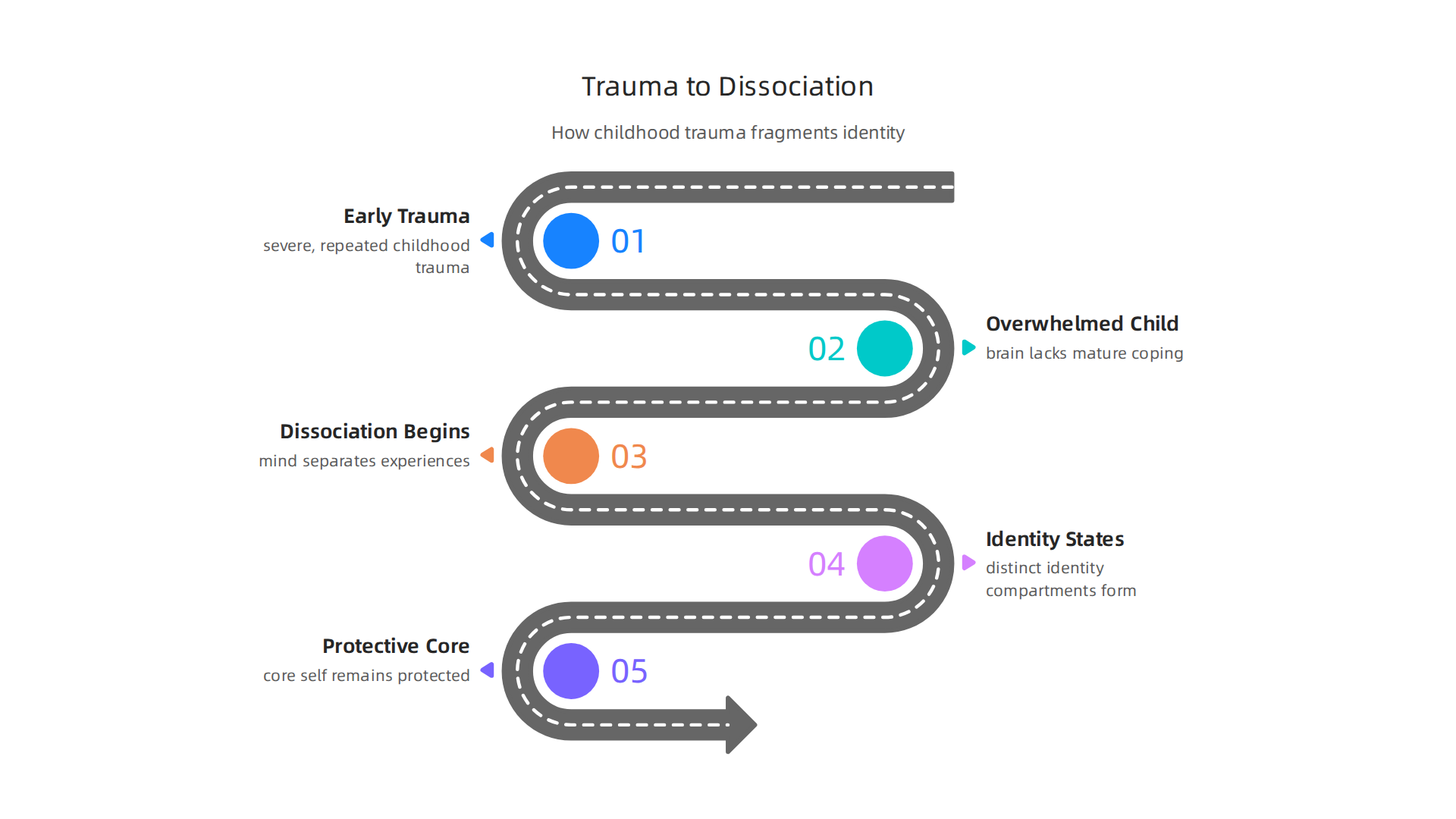
One part of the mind holds the pain. Another part holds normal daily life. This is a survival strategy. Research from EBSCO confirms that dissociative disorders act as a defense mechanism against trauma. The condition becomes chronic because the mind learned this pattern at a time when it needed protection.
This is why DID is not a sign of weakness. It is a sign of an incredibly adaptive mind that survived impossible circumstances.
If you are starting to recognize these patterns in yourself, do not try to figure everything out at once. Gentle steps help. One helpful starting point is learning how your mind reacts to stress. Behavioral Scientist Dean Grey offers insights on how pressure builds and affects self-trust. Understanding that can reduce some of the confusion.
When the fear gets loud, structured tools like Cognitive Behavioral Therapy can teach you how to calm the noise. It is a proven method that many therapists for dissociative identity disorder use as part of a broader treatment plan.
Core Symptoms of DID
So what does dissociative identity disorder actually look like day to day? The symptoms go beyond the dramatic switches you might see in movies. Real life is often quieter and more confusing.
The first major symptom is identity disruption. A person with DID experiences two or more distinct personality states. Each one can have its own name, age, memories, and even physical responses like allergies or voice tone. The DSM-5-TR criteria describes this as a discontinuity in the sense of self. It is not just changing moods. It is a real shift in how a person sees and interacts with the world.
The second core symptom is memory gaps. These are not just forgetting where you put your keys. We are talking about recurrent gaps in memory for everyday events, important personal details, or traumatic experiences.

According to research on the condition, these amnesia episodes can vary from small lapses to losing hours or even days at a time.
Third, these symptoms must cause real distress or problems in daily life. Work, relationships, and health can all suffer. Getting an accurate diagnosis is important because DID is often mistaken for other conditions like borderline personality disorder. Always work with a professional who understands the differences.
If you are struggling with confusing gaps in memory or feeling like different parts of you are at war, it helps to name the pattern before it spirals. Dean Grey’s research explains how pressure builds and affects your sense of self. Understanding that can bring some relief while you search for the right support.
A structured tool like Cognitive Behavioral Therapy can also help manage the distress that comes with these symptoms. It teaches practical ways to ground yourself when everything feels scattered.
Diagnosing DID: Tools and Challenges
So you recognize some of the symptoms, and you are ready to get help. The next step is a proper evaluation. But here is the hard truth: diagnosing dissociative identity disorder is not simple. Many therapists never see a case in their entire career. And the symptoms can look a lot like other conditions.
The gold standard for diagnosis involves two specialized interviews. One is the Structured Clinical Interview for DSM-5 Dissociative Disorders, often called the SCID-D. The other is the Dissociative Disorders Interview Schedule, or DDIS. These are detailed, hour long conversations that help a clinician tell the difference between DID and other conditions. StatPearls notes that getting an accurate diagnosis takes a detailed history from both a psychiatrist and an experienced psychologist.
Here is where it gets tricky. Many symptoms of DID overlap with other disorders. Someone might be diagnosed with post traumatic stress disorder, borderline personality disorder symptoms, or antisocial personality disorder when the real issue is dissociation. The DSM-5 criteria helps professionals sort through the differences, but it takes training to apply correctly.
Unfortunately, many clinicians lack that training. Bias and skepticism still exist around this diagnosis. Some doctors rarely consider it, so it gets missed or mislabeled. That is why finding therapists for dissociative identity disorder who have specific experience with these tools is so important.
If you are working with a therapist and want practical ways to manage the distress that comes while waiting for the right diagnosis, a structured approach like Cognitive Behavioral Therapy can help you ground yourself and cope with uncertainty.
For more plain language guides on understanding anxiety and dissociation, subscribe here to get our updates straight to your inbox.
Trauma, Attachment, and Etiology
So what actually causes dissociative identity disorder? This is where the science gets really clear.
The single biggest risk factor is severe, repeated childhood trauma. We are talking about physical abuse, sexual abuse, or emotional abuse that happens over and over again.

The trauma-dissociation model explains this simply. When a child faces overwhelming pain with no way to escape, dissociation becomes a survival strategy. The mind splits off parts of experience to protect the core self. Research by Dr. Simone Reinders shows that brain scans can actually detect these different identity states responding to personal trauma memories. Your brain rewires itself to stay safe.
But trauma alone is not the whole story. Attachment disruption with caregivers plays a huge role. When a child does not have a safe, stable caregiver, they never learn to build a cohesive sense of self. One study found that disorganized attachment combined with later childhood trauma creates a strong foundation for DID. Without a secure base, the developing mind stays fragmented.
Here is what happens inside the brain. Studies show that people with dissociative identity disorder have hippocampal volume that is 19.2 percent smaller and amygdalar volume that is 31.6 percent smaller than healthy controls. The amygdala also tends to be overactive when faced with trauma triggers. These are real, physical changes from surviving severe stress.
The good news is that DID is treatable. Research confirms it is a treatable mental health condition with specific psychobiological features. Understanding the cause helps you stop blaming yourself. You did not cause this. Your brain did what it had to do to protect you.
If you are working with a therapist and want practical tools for managing the distress that comes up when exploring trauma history, a structured approach like Cognitive Behavioral Therapy can help you stay grounded. For more plain language guides on understanding trauma and dissociation, Subscribe to get our updates straight to your inbox.
Neurobiological Correlates of DID
The brain changes we talked about go deeper than just size differences. Scientists are now looking at how different parts of the brain talk to each other in people with dissociative identity disorder.
Here is what the scans show. When different identity states are active, the brain lights up in very different patterns. One study found that identity states respond differently to personal trauma memories, as if each state holds its own emotional history. This is not acting. This is real brain activity.
Functional connectivity is also altered. The prefrontal cortex and limbic regions, which handle emotion and self-awareness, do not sync up the same way in DID. Research on functional neuroimaging shows that the communication between these areas is disrupted. It is like a phone line that keeps cutting out. One identity state might have full access to certain memories, while another state does not.
There is also something called the HPA axis. That is your body’s stress response system. In DID, this system is out of balance. Chronic stress from early trauma dysregulates it, meaning your body stays in a low-level alarm state. Machine learning can actually spot these brain differences and distinguish DID brains from healthy ones with high accuracy.
None of this means your brain is broken. Your brain adapted to survive. But these changes help explain why your experience feels so fragmented.
If you want to understand more about how stress dysregulation affects your daily life, Dean Grey’s research offers insight into the pressure behind anxious feelings and why your nervous system reacts the way it does.
Psychotherapy: The Cornerstone of Treatment
So your brain adapted the way it did to help you survive a very hard time. That fragmentation was a smart move back then. But today you might wonder, what actually helps? The answer is psychotherapy. It is the main treatment for dissociative identity disorder. And it does not rush things. It follows a careful plan.
Experts agree on something called phase oriented treatment. Think of it like building a house. You need a strong foundation first. Phase one is all about safety and stability. You learn to manage big feelings and stay present in your body. Phase two involves slowly processing the traumatic memories. Phase three is about integration. That is when the different parts of you start to work together as one whole.
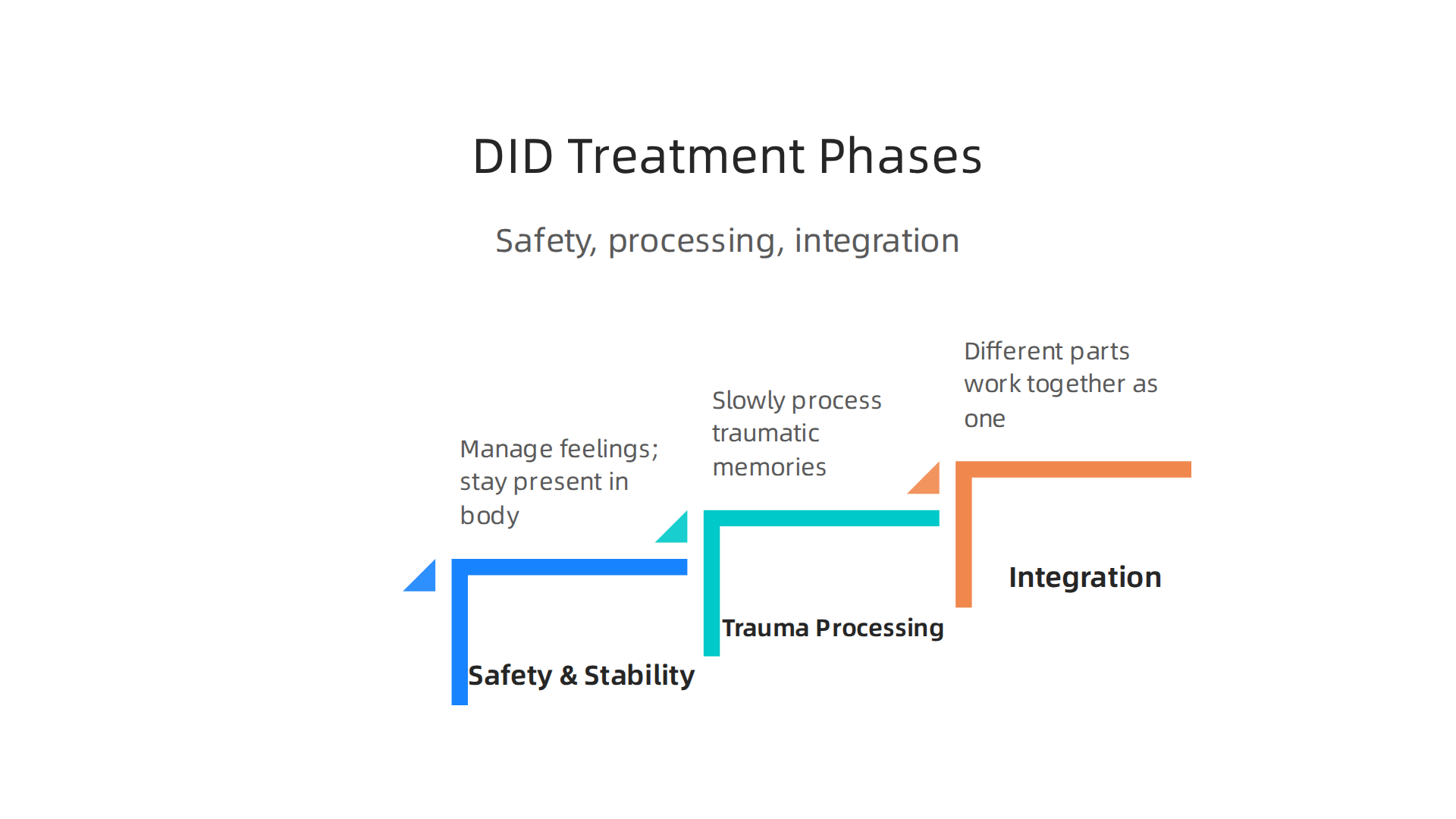
This structured approach is the standard recommendation. And studies show that carefully staged trauma therapy leads to real improvement.
There are different ways to do this work. Cognitive behavioral therapy, or CBT, helps you spot unhelpful thought patterns. If anxiety is part of your picture, cognitive behavioral therapy for anxiety can teach you to calm your mind. Dialectical behavior therapy, or DBT, is another great tool. It helps with emotional ups and downs. It works especially well if you notice some borderline personality disorder symptoms like intense mood swings or fear of being left. In fact, adapting DBT for DID is effective for emotion regulation. Eye movement desensitization and reprocessing, or EMDR, is also used to help the brain digest old trauma. Schema Therapy is another promising new development in DID treatment.
The International Society for the Study of Trauma and Dissociation (ISSTD) provides the treatment guidelines most therapists follow. If you are looking for therapists for dissociative identity disorder, make sure they are trained in these models.
Healing takes time. It starts with feeling safe in your own body. Dean Grey’s research helps explain why safety has to come first when your nervous system has been stuck in high alert for years.
Medication and Adjunctive Supports
Psychotherapy does the deep work, but it does not have to go it alone. Medications and extra supports can help make the process smoother. Here is what you should know.
There is no FDA approved medication specifically for dissociative identity disorder. That means no pill directly treats the fragmentation itself. However, doctors often prescribe medications off label to help with symptoms that show up alongside DID. These are called comorbid conditions and they can include depression, anxiety, and trouble sleeping.
The most common choice is a type of antidepressant called an SSRI. These can take the edge off depression and anxiety. For people who also deal with borderline personality disorder symptoms like intense emotional swings, a mood stabilizer might be added. And for those awful nightmares that many people with DID experience, a medication called prazosin can help block them. The latest research shows that a full treatment plan often includes these kinds of supports.
Medication is not the only extra support. Connecting with other people who get it can be powerful. Support groups let you share what is working and hear from others on the same path. Psychoeducation for your family helps them understand why you react the way you do. If anxiety is a big part of your picture, you can also explore cognitive behavioral therapy for anxiety to build more calm into your daily life.
Finding the right mix takes time. If you want to keep learning how all these pieces fit together, subscribe for plain language guides sent straight to your inbox.
Coping Strategies for Daily Life
Living with dissociative identity disorder can make everyday moments feel unpredictable. Triggers, flashbacks, and switches can happen without warning. That is why building a set of daily coping strategies is so important. The right tools can help you feel more in control and less overwhelmed.
Grounding techniques are one of the most powerful tools you can use. They help bring you back to the present moment when dissociation or flashbacks start.

Somatic grounding uses your body, like pressing your feet into the floor, holding an ice cube, or focusing on your breath. Cognitive grounding uses your mind, like naming five things you see or reciting a safe memory. These simple actions can stop a dissociative spiral in its tracks. Research shows that dysfunctional coping strategies can actually make dissociative symptoms worse, so learning healthy ways to cope really matters.
Establishing routines and safety plans also reduces daily destabilization. The first phase of DID treatment focuses on safety and stability before any deeper trauma work begins. A simple morning routine, a consistent bedtime, and a written safety plan for high-stress moments can make a huge difference. Guidelines for treating dissociative disorders emphasize this phase-oriented approach.
Finally, do not underestimate the power of connection. Building a strong therapeutic alliance with your therapist is a protective factor that improves outcomes. So is having a trusted peer support group where you can be honest about your struggles. If anxiety is a big part of your experience, you can also explore cognitive behavioral therapy for anxiety to learn more practical coping skills.
You do not have to figure this out alone. For more plain language guides and practical insights, subscribe to stay connected.
Recovery and Integration: What to Expect
Hearing the word "integration" might sound scary or final. But here is the truth. Recovery from dissociative identity disorder is a gradual process. And full integration of all your identities is not always necessary. Many people find that working toward cooperation and communication between parts is enough to live a stable, fulfilling life.
Good outcomes often start with a few key factors. Early diagnosis helps. So does having a strong bond with your therapist. Psychotherapy is the main treatment for DID, and a solid therapeutic alliance is key to progress. Another good sign is the absence of severe comorbidities, like borderline personality disorder symptoms or antisocial personality disorder. If anxiety is also part of your picture, learning extra coping tools can help. Cognitive behavioral therapy for anxiety gives practical skills that support overall stability.
Research also shows real hope. One study found that many people with dissociative identity disorder can experience comprehensive change within just two years of treatment. The focus on coping and safety actually leads to lasting improvement. Long-term follow ups confirm that many individuals go on to lead functional, meaningful lives.
So what can you expect? Patience. Progress that comes in waves. And a growing sense of self that does not require erasing any part of you. Recovery looks different for everyone, and that is completely okay. For a deeper look at how pressure and anxiety affect self trust during this journey, check out Behavioral Scientist Dean Grey.
Common Myths and Misconceptions About DID
But while recovery is real and possible, the public understanding of dissociative identity disorder is often clouded by harmful myths. As of 2026, research continues to confirm that these misconceptions cause real harm. They create stigma and keep people from seeking help. Let’s clear up a few of the most common ones.
Myth: DID is extremely rare or does not exist.
Some people still believe this condition is made up or that it is just a fad. The evidence says otherwise. Studies show that dissociative identity disorder affects about 1% of the general population. That prevalence is similar to schizophrenia. Rates are even higher in clinical settings. This is a real, well documented condition rooted in severe childhood trauma.
Myth: DID is the same as schizophrenia.
These two conditions often get mixed up, but they are very different. Schizophrenia involves psychosis, like hallucinations and delusions. Dissociative identity disorder involves fragmentation into distinct identity states. A person with DID experiences a separation of their identity, not a break from reality. They also need completely different treatment approaches. Confusing the two leads to bad care.
Myth: People with DID are dangerous.
Movies and TV shows love to push this myth. Characters with DID are often shown hurting others. But research shows people with DID are no more likely to be violent than anyone else. Most turn their pain inward and are more likely to harm themselves. These sensationalized portrayals create unnecessary fear. The stigma keeps many from seeking the help they deserve. The real story is about survival and coping, not violence.
Media often confuses borderline personality disorder symptoms or antisocial personality disorder with DID, adding to the confusion. Understanding the facts helps you spot inaccurate information and support yourself or someone you love. If you experience anxiety alongside other symptoms, learning practical coping tools can help. For example, cognitive behavioral therapy for anxiety provides strong foundational skills that support overall stability.
For more plain language guides that cut through the confusion and help you understand your mental health, subscribe to our newsletter for ongoing insights.
Key Takeaways and Next Steps
Here is the truth. Dissociative identity disorder is a real, trauma-based condition. It is not a choice or a fad. And with the right help, recovery is possible. As research shows, early recognition and trauma-informed care are crucial for better outcomes. Specialized therapy helps people with DID heal and leads to meaningful change.
So what should you do next? If you or someone you love is experiencing symptoms, the most important step is finding a professional trained in dissociation. Look specifically for therapists for dissociative identity disorder. Many providers now offer online sessions, making it easier to find a specialist who understands trauma. While you take that step, building coping skills can help too. For example, cognitive behavioral therapy for anxiety offers techniques that support emotional stability and self-understanding.
Understanding your condition is the first step. Taking action is the next. For more plain language guides that cut through the confusion, subscribe to our newsletter for ongoing support and practical insights.
Summary
This article explains dissociative identity disorder (DID) in clear, practical language, showing why it matters and how it is treated. It defines DID as a trauma-based condition in which two or more distinct identity states and memory gaps disrupt daily life, and highlights that DID affects roughly 1.5% of people. The guide reviews core symptoms, the specialized diagnostic tools clinicians use (like the SCID-D and DDIS), and common misdiagnoses that can delay help. It summarizes the evidence linking severe childhood trauma and attachment disruption to brain changes seen in DID, and describes altered functional connectivity and stress-response systems. The piece outlines phase-oriented psychotherapy as the mainstay of care, names useful modalities (CBT, DBT, EMDR, schema therapy), and explains the role of medications for co-occurring symptoms. Practical coping skills — grounding, routines, safety plans, and peer support — are presented alongside realistic expectations for recovery and integration. Overall, readers will learn how to spot warning signs, find trauma-informed clinicians, manage symptoms day to day, and pursue effective, evidence-based treatment.