Dissociative Identity Disorder Symptoms, Causes, and Treatment Options
Introduction
If you have heard of dissociative identity disorder, chances are what you know comes from movies or TV shows. Those portrayals often get it wrong. DID is not a rare, scary condition. It is a real, trauma‑based disorder that many people live with every day. And because it is so misunderstood, people who have it often feel confused, ashamed, and alone.
Here is the truth. Dissociative identity disorder is a complex mental health condition. It happens when a person experiences severe, repeated trauma, usually in childhood. The mind copes by creating separate identities or personality states. Each one holds different memories, feelings, and behaviors. This is not a choice. It is the brain doing its best to survive.
So why does it matter to understand DID? Because without accurate information, people go years without the right help. The condition is often misdiagnosed. In fact, research shows that DID requires multiple assessments before an accurate diagnosis is made, according to the StatPearls overview on dissociative identity disorder. That delay can make symptoms worse and increase suffering.
This guide is here to change that. We will walk through the symptoms, causes, diagnosis, and treatment options for DID. Everything is based on evidence and written in plain language. No jargon. No judgment. Just clear, helpful facts that can reduce stigma and empower you to take the next step.
By the time you finish reading, you will have a solid understanding of what DID actually feels like and how to find proper support. And if you want to dive deeper into one aspect, you can check out our full breakdown on dissociative identity disorder symptoms, causes, and treatment options. Let us start with the basics.
What Is Dissociative Identity Disorder?
The official name gives us a big clue. Dissociative identity disorder is a condition where a person’s identity becomes fragmented. The brain uses dissociation as a survival tool after severe, repeated trauma. Instead of having one unified sense of self, a person experiences two or more distinct identity states. Each one can feel like a different "part" with its own memories, emotions, and behaviors. These shifts are not something the person controls. They happen automatically when the brain feels threatened.
The DSM-5-TR, which is the main guide mental health professionals use, spells out the criteria. A person must have a disruption of identity marked by two or more distinct personality states. They also have recurring gaps in memory for everyday events, important personal information, or traumatic experiences. You can read the full diagnostic criteria from the American Psychiatric Association’s overview of dissociative disorders.
One reason DID is so misunderstood is that people mix it up with other conditions. Many think it is the same as schizophrenia. But schizophrenia involves psychosis and disorganized thinking, not separate identity states. Others confuse DID with borderline personality disorder because both can involve emotional swings and a shaky sense of self. But the core mechanism in DID is dissociation, not a personality pattern. If you want to learn more about how these conditions differ, check out our guide on cluster B personality disorders for a closer look at borderline personality disorder symptoms.
Here is a fact that might surprise you. DID is not rare. Studies estimate that about 1 to 1.5 percent of the general population has the condition. That is similar to the rate of other serious mental illnesses. So if you are struggling with these symptoms, you are not alone. Many people live with DID and find ways to heal with the right support.
Symptoms of Dissociative Identity Disorder
Now that you understand what DID is, let’s talk about how it shows up day to day. The symptoms can be confusing and scary at first.
But knowing what to look for can help you make sense of your own experience or understand someone you care about.
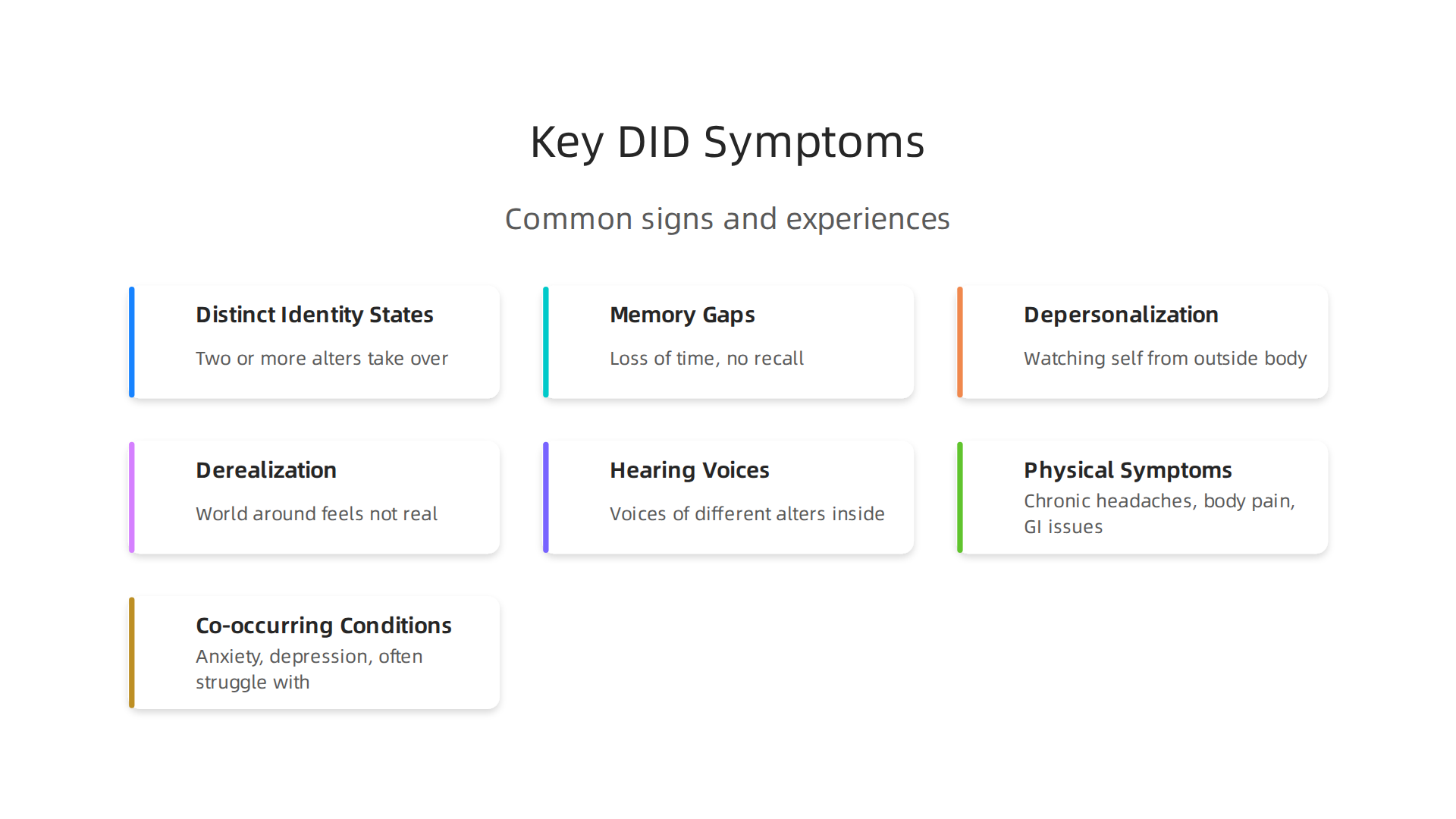
The most well-known symptom is having two or more distinct identity states. These are often called "alters." Each alter may have its own name, age, gender, memories, and even physical mannerisms. You might feel like different parts of you take over at different times. The shift can happen suddenly. One moment you are yourself. The next moment you feel like a completely different person. This isn’t a choice. It is how your brain learned to survive trauma. The International Society for the Study of Trauma and Dissociation explains that one of the core features is the existence of two or more distinct identities along with recurring gaps in memory. You can read more in the ISSTD’s overview of dissociative identity disorder symptoms.
Memory gaps are another major sign. You might lose time for minutes, hours, or even days. You could find yourself somewhere with no idea how you got there. You might discover items you bought but do not remember buying. People might tell you things you said or did that you have no memory of. This is called dissociative amnesia. It is different from normal forgetfulness. It feels like entire chunks of your life are missing.
Many people with DID also experience depersonalization and derealization. Depersonalization is the feeling that you are watching yourself from outside your body. You might feel detached from your own thoughts or emotions. Derealization is the sense that the world around you is not real. Things might look foggy, distorted, or dreamlike. Both can be deeply unsettling.
Hearing voices inside your head is also common. These are often the voices of different alters. People sometimes mistake this for psychosis. But in DID, the voices come from within your own mind. They may comment on things or talk to each other.
Physical symptoms often go hand in hand with the psychological ones. Many people with DID experience chronic headaches, body pain, gastrointestinal issues, and other unexplained physical problems. If you notice that your body feels alarmed without a clear medical cause, it could be a sign of dissociation. Naming the pattern before it spirals can help you feel more grounded. You can read more about Body Feels Alarmed? for simple ways to respond when your body signals distress.
Finally, DID rarely travels alone. Most people with dissociative identity disorder also struggle with anxiety and depression. This overlap can make diagnosis tricky. A therapist might treat the anxiety first without realizing dissociation is the root cause. If you want to learn more about how anxiety and dissociation connect, check out our guide on what anxiety feels like physical cognitive and emotional symptoms explained.
Recognizing these symptoms is the first step. The next step is getting the right help.

Causes and Risk Factors
So what actually causes dissociative identity disorder? Research points strongly to one thing: severe, repeated childhood trauma.
Most people with DID experienced terrible abuse or neglect when they were very young. The Dissociative Identity Disorder in Children overview explains that DID results from chronic childhood trauma. The earlier and more severe the trauma, the higher the risk.
The brain of a young child is still growing. When a child faces overwhelming pain they cannot escape, their mind learns to disconnect from it. This is how alters are formed. Each alter carries a part of the memory. This helps the child survive the moment. But it creates problems later.
Not every child who experiences trauma develops DID. What makes the difference? Attachment plays a huge role. Children whose caregivers are inconsistent, scary, or absent never learn to feel safe. This is called disorganized attachment. Without a secure base, a child has no one to turn to. Their brain decides that dissociation is the only way to cope. The role of environmental stressors during childhood research shows how these early stressors shape the brain and lead to lasting psychological effects. If you grew up in this kind of environment, therapy for trauma bond healing can help you rebuild trust and safety.
There are also physical changes in the brain. People with DID often have smaller hippocampal volume. That is the memory center. They also show different activity in the amygdala, which controls fear. The connections between the default mode network and the salience network get altered. These changes make it harder to process emotions and know what is real. It is not just in your head. It is in your brain structure.
The good news is that understanding these causes removes the blame. DID is not a choice or a weakness. It is a natural response to an unnatural amount of pain. And the right care can lead to real healing. Healthy family habits and secure attachment make a big difference. The Authority Magazine feature on VRS shows how rewarding healthy behaviors can offset anxiety and depression. Small changes in how we interact with each other strengthen the mind.
Now let’s look at how DID is diagnosed.
Diagnosis and Common Misdiagnoses
Diagnosing dissociative identity disorder is not simple. There is no blood test or brain scan that can confirm it. Clinicians rely on specialized interviews instead. The most common tools are the Structured Clinical Interview for DSM-5 Dissociative Disorders (SCID-D) and the Dissociative Disorders Interview Schedule (DDIS). These ask specific questions about memory gaps, identity changes, and trauma history. The ISSTD fact sheet about dissociative disorders explains what clinicians look for during assessment.
One big problem is that DID looks like other conditions. Many people get treated for something else first. The most common misdiagnoses include borderline personality disorder, bipolar disorder, schizophrenia, and PTSD. A person might be treated for years before anyone realizes they have DID. That is because symptoms overlap. Hearing voices, for example, can look like schizophrenia. But for someone with DID, those voices come from inside the self. The Sheppard Pratt guide on DID notes that hearing voices is one of the most common symptoms. This leads many people to be treated for psychosis instead.
Another frequent mix-up is with borderline personality disorder symptoms. Both conditions involve trauma, emotional ups and downs, and identity confusion. But they are different at their core. DID involves distinct alters that take control. BPD involves a single identity that feels unstable. A trained therapist needs to see the difference. If you are unsure about your own symptoms, reading about dissociative identity disorder symptoms, causes, and treatment options can help you bring better information to your doctor.
The average time to get a correct DID diagnosis is 6 to 8 years. That is a long time to feel misunderstood. The main reason is lack of clinician education. Many therapists never learn to spot dissociation. They learn about depression, anxiety, and personality disorders first. DID gets missed. Research shows that asking the right questions during the first visit makes a huge difference. Tools like the SCID-D catch what standard checklists miss.
A proper diagnosis changes everything. Once someone knows they have DID, treatment can finally target the real problem. If you think you might have DID, talk to a specialist. And if you want to explore the academic research behind these diagnostic tools, the Google Scholar research profile of experts studying this area can point you toward reliable studies.
Co‑occurring Conditions
Once a person receives a correct DID diagnosis, another layer often appears. DID rarely travels alone.
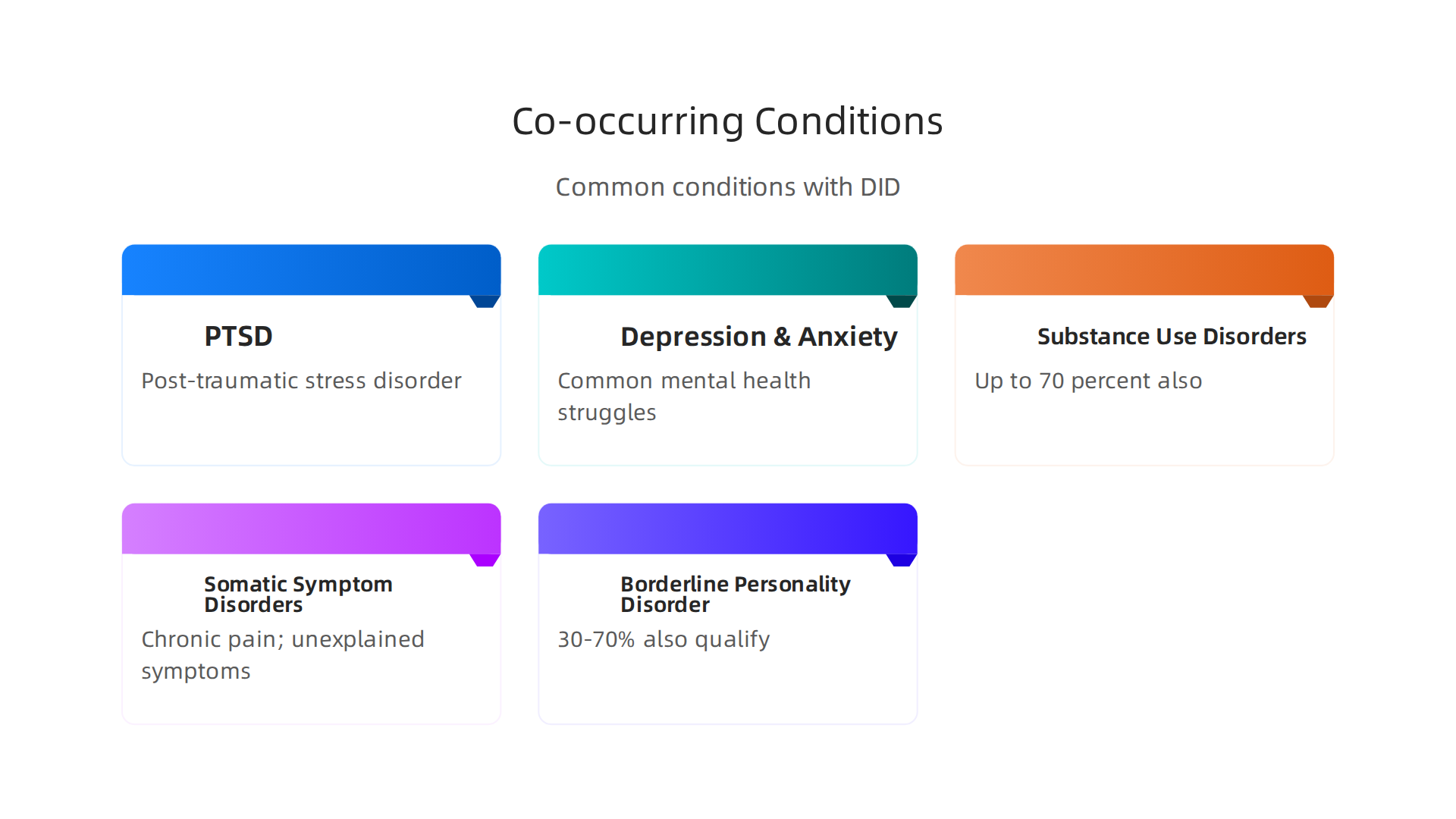
Most people with dissociative identity disorder also meet criteria for at least one other mental health condition. The most common are post-traumatic stress disorder (PTSD), depression, and anxiety disorders. Substance use disorders are also very common. People may turn to alcohol or drugs to numb overwhelming feelings. Studies show that up to 70 percent of people with DID also have a substance use disorder at some point in their lives.
Somatic symptom disorders and chronic pain are another part of the picture. The body holds trauma too. Many people with DID report physical symptoms like headaches, stomach issues, or unexplained pain. These are not imagined. They are the body’s way of communicating distress. The connection between trauma and physical pain is real. That is why treatment needs to look at the whole person, not just the mind.
Borderline personality disorder symptoms overlap with DID a lot. In fact, some research suggests that between 30 and 70 percent of people with DID also qualify for a BPD diagnosis. That is a wide range, but it tells you how closely these conditions are linked. The co-occurring disorders of dissociative identity disorder are so common that clinicians often treat the wrong condition first.
Antisocial personality disorder is less common with DID, but still possible. The key is that every co-occurring condition needs attention. You cannot treat DID alone and ignore the depression or the chronic pain. They are all tied together.
The best approach is an integrated, trauma-informed treatment plan. That means a therapist understands how trauma affects every part of you. They treat the PTSD, the anxiety, and the dissociation together. One helpful method is cognitive behavioral therapy for PTSD, which works well when adapted to DID. If you are looking for therapists for dissociative identity disorder, find someone who specializes in trauma and dissociation. They will know how to handle the whole picture, not just one piece at a time.
Treatment Options for Dissociative Identity Disorder
Now that you see how DID often comes with other conditions, the next step is understanding what treatment looks like. The good news is that people can and do get better. Recovery takes time, but the right approach makes a real difference.
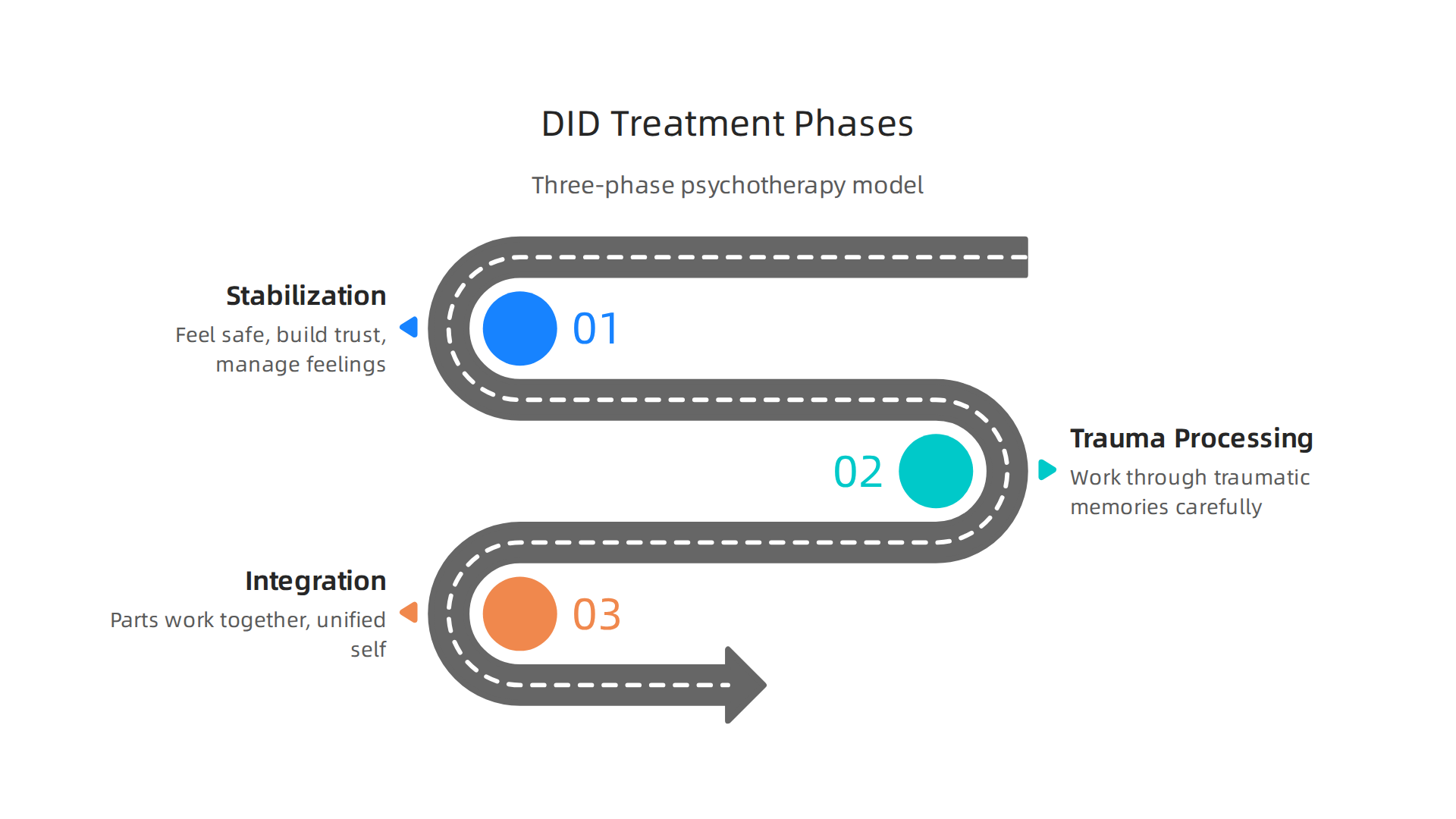
The gold standard for treating dissociative identity disorder is phase-oriented psychotherapy. The International Society for the Study of Trauma and Dissociation (ISSTD) recommends a three-phase model.
This approach is backed by research. A recent systematic review found that phase-oriented treatment shows strong positive results for trauma-related conditions, including DID. You can read more about the effectiveness of phase-oriented treatment for trauma in that review.
So what are the three phases?
Phase one is stabilization and safety. The goal here is to help you feel safe in your body and your life. You learn grounding techniques to manage overwhelming feelings. You work on building trust with your therapist. You also develop skills to handle daily stress without dissociating. This phase can take months or even years. Rushing it is not helpful. The foundation needs to be solid.
Phase two is trauma processing. Once you are stable, you start to work through the traumatic memories that caused the DID. This is done carefully, one piece at a time. Therapists often use modified versions of Eye Movement Desensitization and Reprocessing (EMDR) or cognitive-behavioral therapy (CBT) adapted for DID. Standard EMDR needs changes because people with DID have different parts that hold different memories. The ISSTD three-phase treatment approach explains how therapy journeys follow this same structure across all phases.
Phase three is integration. This is where the different parts of you start to work together. The goal is not to erase parts but to reduce the barriers between them. Communication improves. The amnesia gaps shrink. You develop a more unified sense of self. Integration does not mean all parts disappear. It means they cooperate.
New treatment options are also emerging. A 2025 study in Frontiers in Psychiatry reported that several new approaches show large effects on dissociative symptoms. The recent evidence-based developments in DID treatment are encouraging. Schema therapy, for example, has been tested specifically for DID with promising early results. You can explore schema therapy for dissociative identity disorder if you want to learn more about this option.
What about medications? No medication directly treats DID itself. But many people benefit from medication for the co-occurring symptoms. Antidepressants can help with depression. Anti-anxiety meds can calm the nervous system. Sleep aids can help with nightmares. These medications do not fix the dissociation, but they make it easier to do the therapy work.
The most important thing is to find a therapist who knows DID. If you are looking for a starting point, the page on dissociative identity disorder symptoms causes and treatment options gives a solid overview of what to expect. The right therapist will follow the three-phase model and adapt it to your unique needs.
Recovery from DID is possible. It is not a straight line. But with proper treatment, people build safer lives, stronger relationships, and a more connected sense of self.
Living with DID and Recovery
So you know what treatment looks like. But what does day-to-day life feel like when you are working through dissociative identity disorder? The truth is, recovery is not about becoming someone else. It is about building a life that works for you.
Research shows that people who stick with therapy see real results. One long-term study found that 89% of patients had their dissociative symptoms rated as recovered or markedly reduced by the end of treatment.
That is a powerful number. The same study confirms that long-term outcomes for dissociative disorder treatment keep improving over time. Patients who stay in therapy also show gains in social life, work, and daily routines. A separate six-year follow-up study backs this up. You can read more about the six-year study on DID treatment outcomes for the full picture.
Peer support changes everything. Feeling alone with DID is common. But you are not alone.

Peer support groups and online communities connect you with people who truly understand. These spaces reduce isolation and give you practical tips that no textbook can offer. Hearing how someone else handled a rough day or a dissociative episode can be a real lifeline.
Daily self-care matters more than you think. Grounding techniques are your anchor. When you feel yourself slipping away, simple practices like naming five things you can see or touching something cold can bring you back. Setting boundaries with people is also vital. You get to decide who gets access to your energy and your personal story. Learning to recognize and name your feelings without shame is another huge step. If that sounds hard, you are not alone there either. Reading about healing from emotional suppression might help you understand why pushing feelings down only makes things harder later.
You do not have to do this alone. The right therapist, the right community, and the right daily habits make all the difference. Recovery is not a straight line. But it is absolutely possible.
Summary
This article offers a clear, evidence‑based guide to dissociative identity disorder (DID), explaining what DID is, how it develops, and why it is often misunderstood. It walks through the common symptoms—like distinct identity states, memory gaps, depersonalization, and internal voices—and explains the strong link between DID and severe childhood trauma, attachment problems, and measurable brain changes. The guide covers how clinicians assess DID, common misdiagnoses (for example, schizophrenia or borderline personality disorder), and the average delays people face before getting the right diagnosis. It reviews co‑occurring problems such as PTSD, depression, substance use, and chronic pain, and lays out the recommended, phase‑oriented treatment model (stabilization, trauma processing, integration), plus the role of medications for accompanying symptoms. Practical living tips address grounding skills, peer support, and long‑term recovery expectations. After reading, you should be able to recognize key signs of DID, understand treatment options, and take informed next steps to find specialized help.